The Cranial Cruciate Ligament: Injuries and Repair

Understanding Canine Cruciate Ligaments
Canine cruciate ligaments are vital structures within a dog’s knee joint, responsible for stabilizing the joint and ensuring smooth, efficient movement. Cruciate ligaments are present in pairs, and together make the knee a hinge joint. Specifically, the cranial cruciate ligament (CCL) is crucial for maintaining the alignment of the femur and tibia bones in dogs, preventing abnormal motion that can lead to knee instability and pain. Injury to the cranial cruciate ligament is one of the most common orthopedic issues in dogs. The cruciate ligaments do not have a good blood supply, and will not heal, therefore, requiring surgical intervention. The surgeons at Animal Outpatient Surgery of San Diego (AOSSD) are highly experienced in treating damaged cruciate ligaments, having successfully performed thousands of procedures. Trusted by fellow veterinarians for their expertise, AOSSD is a leading authority in canine cruciate ligament repair.
The video below explains TPLO surgery in more detail and helps pet owners understand the surgical process in greater detail.
How does the cruciate ligament get damaged and how can I tell?
Damage to the canine cruciate ligament can occur due to various factors, including acute trauma, degenerative cruciate disease in dogs, and genetic predisposition. Activities that involve sudden stops, jumps, or twists can lead to a canine torn cruciate ligament, commonly referred to as a dog CCL injury. Breeds such as Pitbulls, Labrador Retrievers, Rottweilers, and German Shepherds are particularly prone to this injury, which may occur after normal activity in these breeds that experience the degenerative form of the disease.
You may notice several symptoms indicating a cranial cruciate ligament injury, such as limping, difficulty bearing weight on the affected leg, swelling around the knee, and decreased activity levels. While these signs can suggest a potential CCL injury, a definitive diagnosis requires evaluation by a qualified veterinarian. At AOSSD, our surgeons use history, orthopedic physical exam and digital radiography to assess the extent of the damage, and to verify the diagnosis. These images help vet surgeons look for signs of joint effusion, bone spurs, and the position of the tibia relative to the femur.

Pre Op TPLO Radiographs TPA ( Tibial plateau angle) of 29 degrees

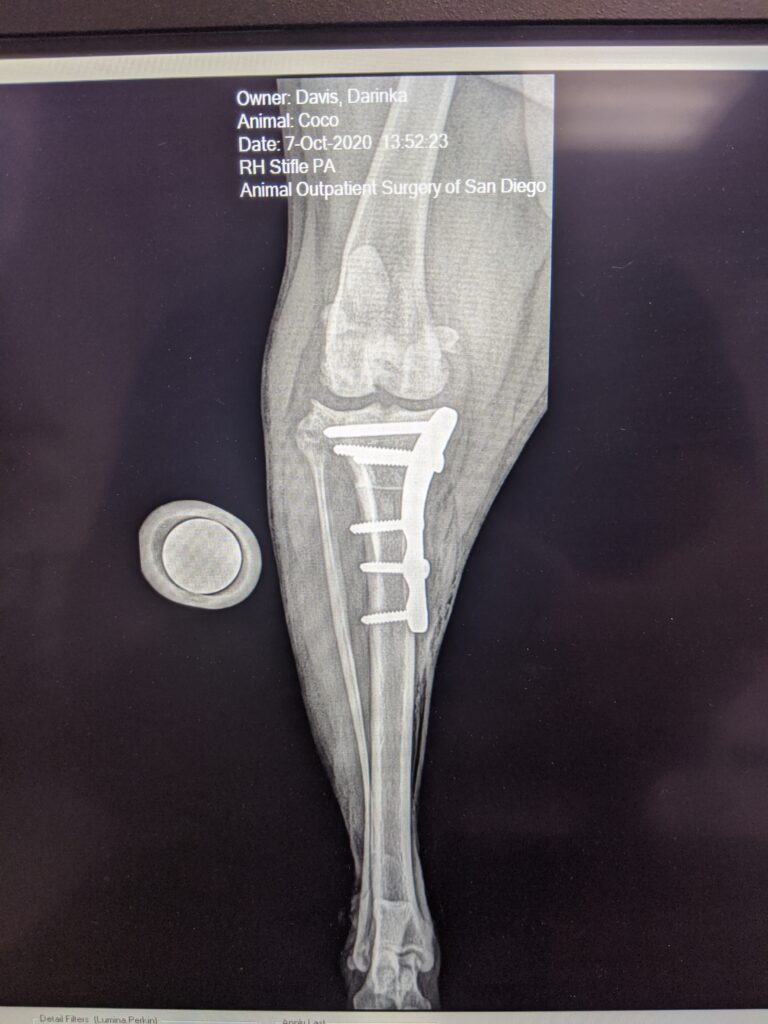
Post Op TPLO front view
What treatment options are available?
The treatment of canine cruciate ligament injuries depends on the severity of the damage and the individual dog’s circumstances, such as age, size, weight, and activity level. Treatment options range from conservative management to surgical intervention.
Conservative Management:
For very mild cases or when surgery is not immediately feasible, conservative methods may be employed. These include rest, activity restriction, and administration of dog-safe anti-inflammatories to manage pain and inflammation. Weight management and controlled physical therapy can also support joint health and recovery.
Surgical Options:
In most cases CCL dog surgery becomes necessary. Three common surgical techniques are Tibial Plateau Leveling Osteotomy (TPLO), Tibial Tuberosity Advancement (TTA), and Lateral Suture (LS). Both TPLO and TTA aim to stabilize the knee joint by altering the dynamics of the tibia to prevent abnormal motion and pain. LS is a procedure that stabilizes the knee joint by placing a strong, synthetic suture material around the knee’s lateral (outer) aspect. This suture mimics the function of the damaged cranial cruciate ligament, preventing the tibia from moving forward relative to the femur, which is the primary issue when the CCL is ruptured. The choice between TPLO, TTA, and TS depends on the specific needs of the dog and should be made in consultation with a qualified veterinarian.
How do I look after my dog post-op?
Post-operative care is crucial for a successful recovery from cruciate ligament surgery. Key aspects of post-op care include rest, restricted activity, and pain management. You should follow your veterinary surgeons’ recommendations closely, ensuring your dog avoids strenuous activities and adheres to prescribed medication schedules. The recovery period can vary, but it typically takes 16 or more weeks for your dog to regain full function. For detailed post-op care instructions, pet owners can refer to AOSSD’s post-op guide.
How can I prevent cruciate ligament injury?
Preventive measures can potentially reduce the risk of cruciate ligament injuries and knee problems in dogs. Maintaining a healthy weight through a balanced diet and regular exercise is essential, as excess weight places additional stress on the joints. Avoiding high-impact activities that involve abrupt stops and jumps can also help protect the ligaments. Regular veterinary check-ups are important to monitor joint health and detect potential issues early.

Our professional opinion
After 25 years of performing canine cranial cruciate ligament repair, Dr. Farrell and the team have certainly formed some opinions that may help you as you consider your course of treatment. First, the choice to have surgery is most important. The cruciate ligament has negligible blood supply and does not heal, and therefore, surgical treatment is indicated. Next, if your dog is over 10 lbs and active, they will likely do best with a TPLO, and return to full function most quickly. If your dog is 10 lbs or under, a lateral suture has a 99% chance of working wonderfully. If your dog is quite elderly, or has other medical issues limiting mobility, a lateral suture can be a more economic and effective repair as compared to TPLO. TTA has specific limitations which can be discussed at your appointment. A consultation with our surgeon to discuss your pet’s individual needs is the best plan to determine the recommended surgery for your pet.
Contact us for our professional opinion regarding conservative and surgical treatments for your dog’s cruciate ligament problems.